Anabolic-Androgenic Steroids

A Visual Forensic Guide to Ten Prevalent Compounds
Pharmacokinetics, detection science, clinical profile, and litigation use for attorneys, judges, and forensic professionals
By ToxGirl
| The legal point: AAS cases are rarely won or lost on the label “steroid.” They turn on compound identity, detection window, confirmation method, dose/timeline fit, and whether the expert can distinguish exposure from impairment or recent use. |
Introduction
Anabolic-androgenic steroids (AAS) occupy a uniquely difficult space in forensic toxicology. They are legitimate therapeutic agents in some contexts, regulated controlled substances in others, and common performance-enhancing drugs in athletics and general-population misuse.
For legal professionals, the science cannot be reduced to a positive/negative label. Testosterone is endogenous and requires isotope-ratio confirmation. Nandrolone can remain detectable long after use. Oral 17-alpha alkylated compounds create liver-risk questions distinct from injectable esters. Veterinary-only drugs such as trenbolone and boldenone raise a different forensic inference than FDA-approved medications.
This revised article converts the original compound-by-compound guide into a visual litigation reference: a fast comparison chart, detection-window graphics, a toxicological risk heat map, and a practical attorney checklist.
Key Takeaways for Legal Professionals
- All ten compounds discussed here are controlled AAS; the legal analysis still requires compound-specific toxicology rather than class-wide generalizations.
- Detection windows vary from roughly three weeks to 12-18 months, which makes timeline reconstruction central in any prosecution, sanction, employment action, or expert report.
- Anabolic and androgenic ratings are derived from bioassays and are not direct evidence of human impairment, intent, aggression, or behavioral change.
- Testosterone requires C-IRMS confirmation because it is endogenous; a T/E ratio alone is an investigative trigger, not a complete forensic conclusion.
- Trenbolone has no FDA-approved human use; any confirmed human detection is exogenous, but that still does not automatically prove timing, dose, or impairment.
- Oral 17-alpha alkylated compounds – especially oxymetholone, stanozolol, and methandrostenolone – raise hepatotoxicity issues that differ from most injectable esters.
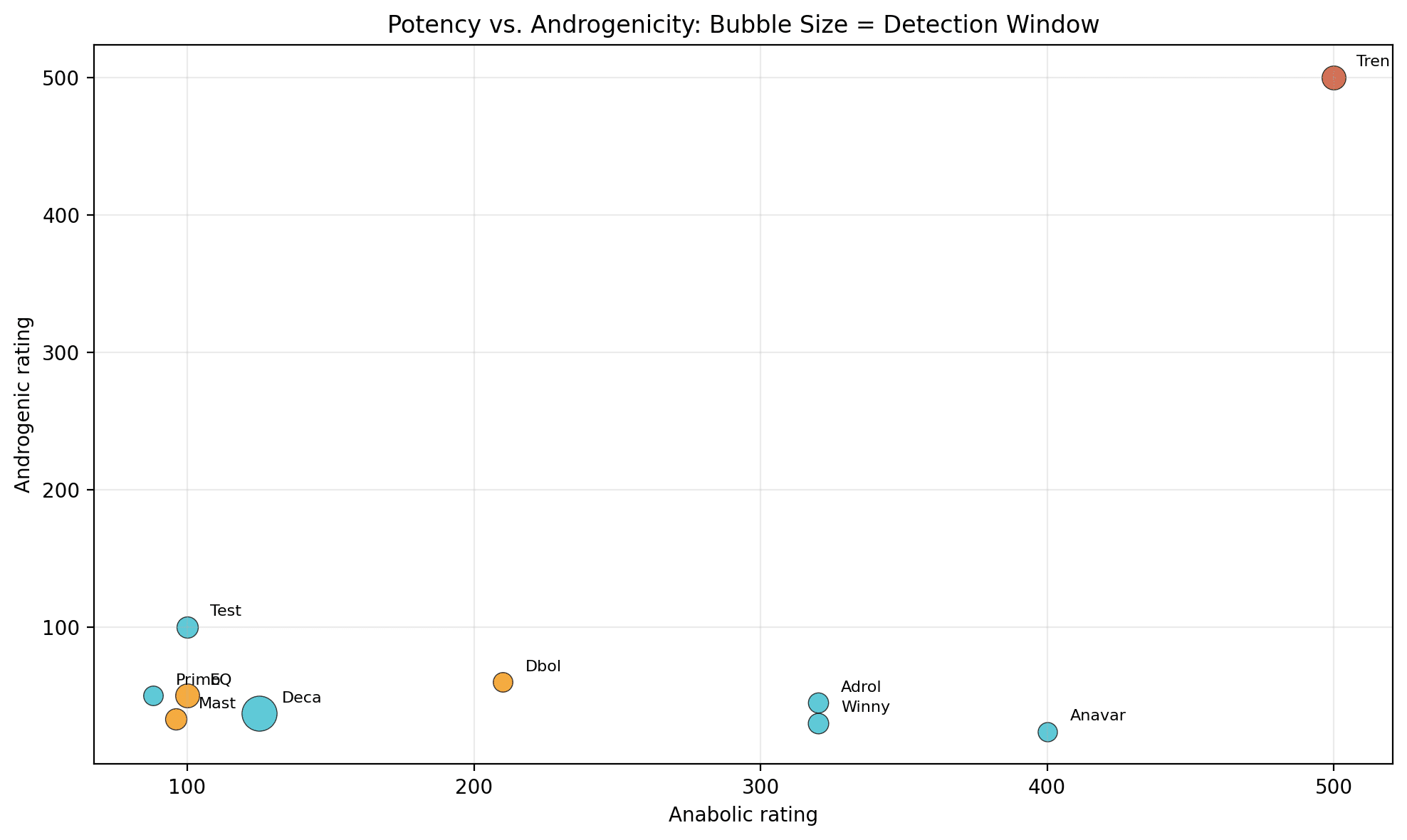
Visual Summary: What Changes the Litigation Analysis?
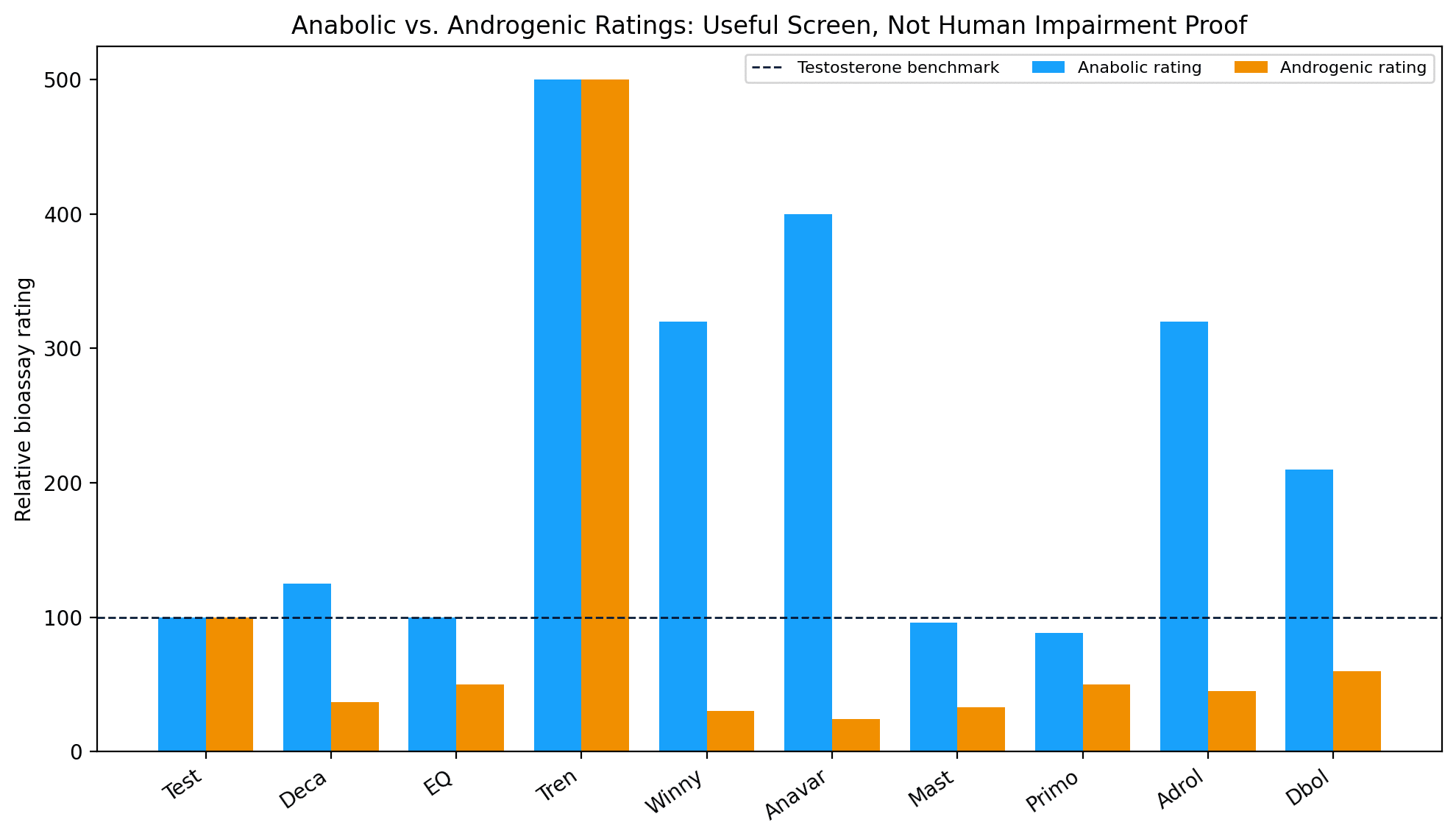
| Interpretation: The ratings are best used as a relative pharmacology screen. They should not be converted into courtroom claims of impairment, aggression, or recent use without compound-specific human data and case-specific facts. |
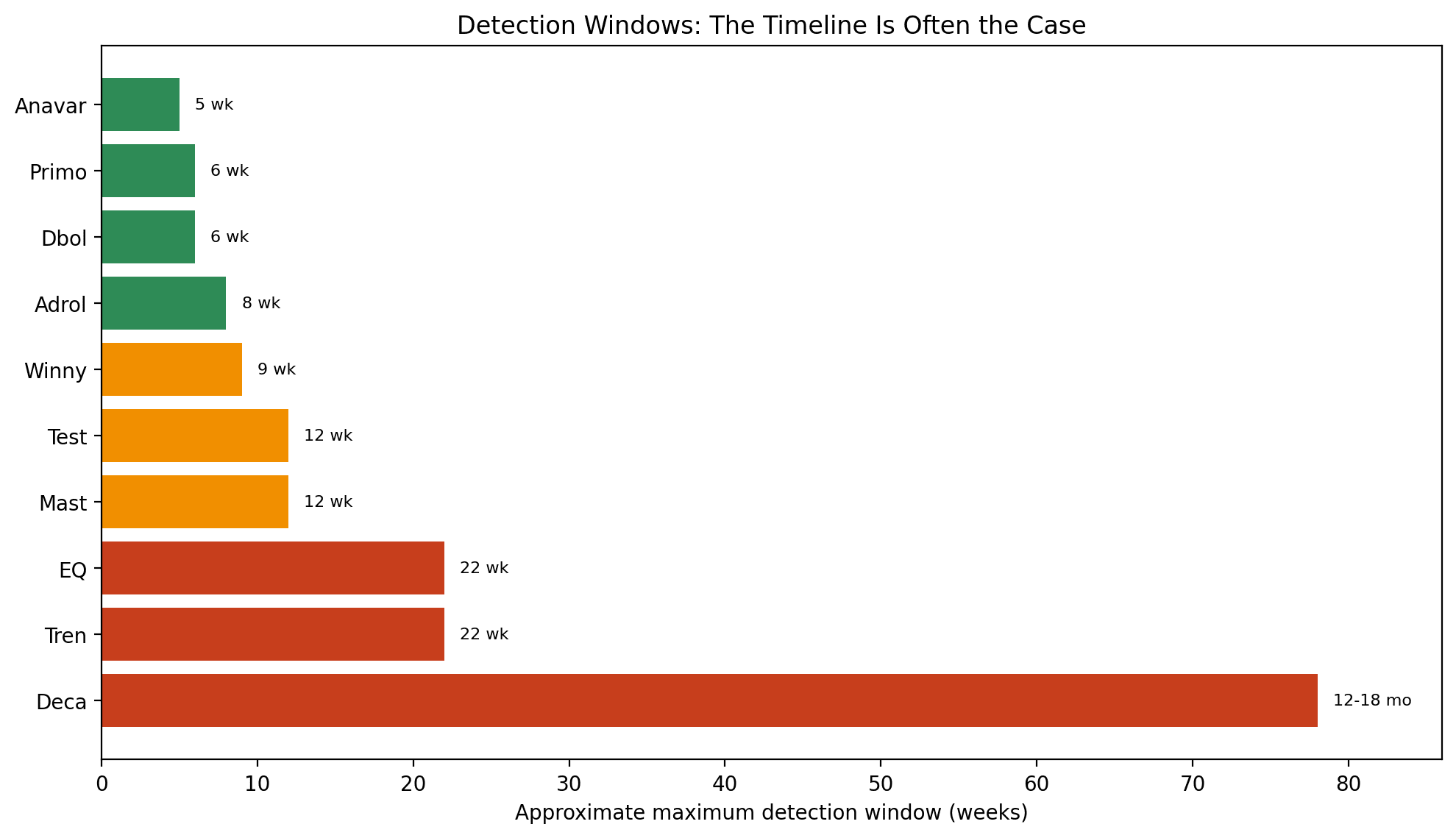
| Timeline warning: A long detection window can prove past exposure while saying little about when use occurred. Nandrolone is the classic example: detection can persist far beyond any alleged acute effect. |
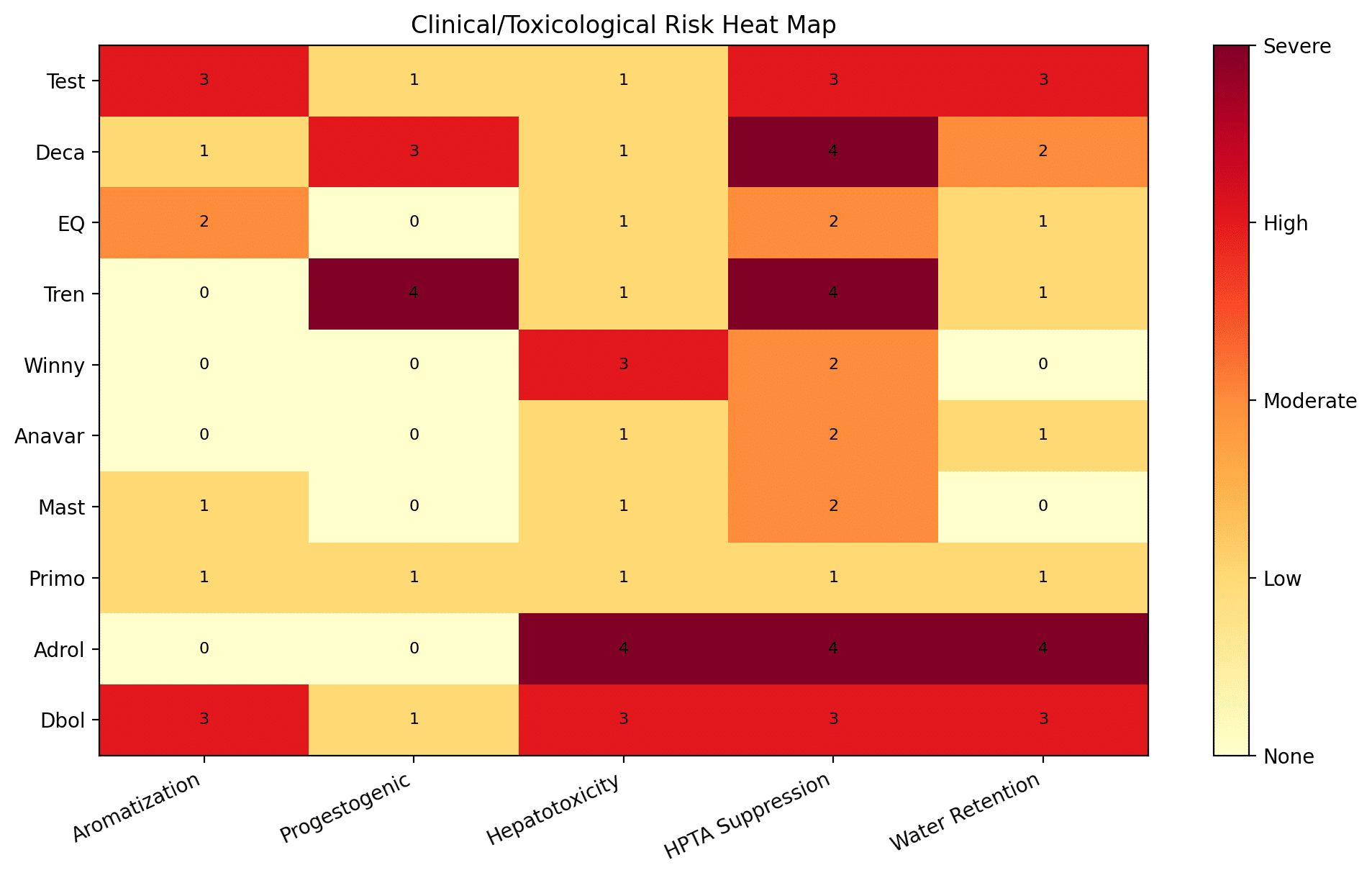
| Risk map key: 0 = none, 1 = low/minimal, 2 = moderate, 3 = high/significant, 4 = severe/very high/extreme. Scores summarize the article’s qualitative categories and are intended as visual triage, not medical diagnosis. |
Part I: The Science Beneath the Label
What “Anabolic-Androgenic” Means
Every compound in this guide acts primarily through the androgen receptor, a nuclear transcription factor present in muscle, bone, liver, brain, prostate, and other tissues. Binding can alter protein synthesis, nitrogen retention, erythropoiesis, bone density, and secondary sex-characteristic signaling.
“Anabolic” generally refers to tissue-building effects, especially skeletal muscle. “Androgenic” refers to masculinizing effects, including prostate activity, sebaceous gland effects, virilization, and hair-loss risk in susceptible individuals. The two effects cannot be fully separated because they proceed through the same receptor system.
| Courtroom translation: A high anabolic:androgenic ratio does not equal proof of strength increase, aggression, intoxication, or impairment in a particular human being. It is a historical comparative measure, not a clinical verdict. |
Structural Families That Matter
19-nor compounds: Nandrolone and trenbolone lack the C-19 methyl group. This changes metabolism and often increases progestogenic relevance. Both can strongly suppress the HPTA.
DHT-derived compounds: Stanozolol, oxandrolone, drostanolone, and methenolone are resistant to aromatization and have distinct androgenic profiles.
17-alpha alkylated oral compounds: Stanozolol oral, oxandrolone, oxymetholone, and methandrostenolone are orally bioavailable but carry hepatic-risk issues because the C-17 modification resists first-pass metabolism.
Testosterone-derived compounds: Boldenone is structurally close to testosterone, but the C-1,2 double bond and undecylenate ester alter aromatization, release, and metabolite interpretation.
The Ester System
Many injectable AAS are esterified at the C-17 hydroxyl group. After intramuscular injection, the ester acts as a depot. Lipases cleave the ester and release active steroid over days to weeks. Long-chain esters such as decanoate, undecylenate, and enanthate generally produce slower release and longer detection windows; short esters such as propionate and acetate peak and clear faster. This is why route, ester, dose, and chronicity are central to timeline analysis.
Part II: Compound Profiles – Litigation-Relevant Summary
Testosterone (Test)
| Anabolic | Androgenic | Max Detection | Aromatization | Hepatic Risk | FDA Approved |
| 100 | 100 | ~12 wk | High | Low | Yes |
Reference standard; endogenous; IRMS required
Forensic emphasis: because testosterone is endogenous, exogenous use requires C-IRMS confirmation. A T/E ratio is an investigative flag, not a stand-alone forensic conclusion.
Nandrolone Decanoate (Deca)
| Anabolic | Androgenic | Max Detection | Aromatization | Hepatic Risk | FDA Approved |
| 125 | 37 | 12-18 mo | Low | Low | Yes |
Longest detection window; 19-NA metabolite
Forensic emphasis: the extraordinarily long 19-norandrosterone detection window is powerful for exposure evidence but dangerous if misused as proof of recent use or current effect.
Boldenone Undecylenate (EQ)
| Anabolic | Androgenic | Max Detection | Aromatization | Hepatic Risk | FDA Approved |
| 100 | 50 | ~22 wk | Low-Mod | Low | No |
Veterinary compound; hematocrit/polycythemia issue
Forensic emphasis: do not treat this compound as interchangeable with testosterone or any other AAS. The ester, metabolite, and adverse-effect profile control the analysis.
Trenbolone (Tren)
| Anabolic | Androgenic | Max Detection | Aromatization | Hepatic Risk | FDA Approved |
| 500 | 500 | ~22 wk | None | Low | No |
No human indication; any detection is exogenous
Forensic emphasis: no FDA-approved human indication makes confirmed detection exogenous, but the expert must still address timing, dose, method, and behavioral relevance.
Stanozolol (Winny)
| Anabolic | Androgenic | Max Detection | Aromatization | Hepatic Risk | FDA Approved |
| 320 | 30 | ~9 wk | None | High | Yes |
Oral vs depot timelines differ; HDL/tendon risk
Forensic emphasis: the 17-alpha alkylated oral class creates hepatic and lipid-risk issues, but route and timing still require compound-specific proof.
Oxandrolone (Anavar)
| Anabolic | Androgenic | Max Detection | Aromatization | Hepatic Risk | FDA Approved |
| 400 | 24 | ~5 wk | None | Mild | Yes |
Safer oral AAS profile, still 17-AA
Forensic emphasis: the 17-alpha alkylated oral class creates hepatic and lipid-risk issues, but route and timing still require compound-specific proof.
Drostanolone (Mast)
| Anabolic | Androgenic | Max Detection | Aromatization | Hepatic Risk | FDA Approved |
| 96 | 33 | ~12 wk | Anti-E | Low | No |
DHT-derived; mild anti-estrogenic activity
Forensic emphasis: do not treat this compound as interchangeable with testosterone or any other AAS. The ester, metabolite, and adverse-effect profile control the analysis.
Methenolone (Primo)
| Anabolic | Androgenic | Max Detection | Aromatization | Hepatic Risk | FDA Approved |
| 88 | 50 | ~6 wk | Minimal | Low | Yes |
Low suppression and low hepatic burden
Forensic emphasis: do not treat this compound as interchangeable with testosterone or any other AAS. The ester, metabolite, and adverse-effect profile control the analysis.
Oxymetholone (Adrol)
| Anabolic | Androgenic | Max Detection | Aromatization | Hepatic Risk | FDA Approved |
| 320 | 45 | ~8 wk | None* | Severe | Yes |
Most hepatotoxic oral; paradoxical estrogenic effects
Forensic emphasis: the 17-alpha alkylated oral class creates hepatic and lipid-risk issues, but route and timing still require compound-specific proof.
Methandrostenolone (Dbol)
| Anabolic | Androgenic | Max Detection | Aromatization | Hepatic Risk | FDA Approved |
| 210 | 60 | ~6 wk | High | High | No |
Classic oral AAS; hepatotoxic and estrogenic
Forensic emphasis: the 17-alpha alkylated oral class creates hepatic and lipid-risk issues, but route and timing still require compound-specific proof.
Part III: Side-by-Side Comparison Tables
| Compound | Anabolic | Androgenic | Max Detection | Aromatizes | Progestogenic | Hepatotoxic | HPTA | Water | FDA |
| Test | 100 | 100 | 12 wk | High | Low | Low | Significant | High | Yes |
| Deca | 125 | 37 | 12-18 mo | Low | High | Low | Severe | Moderate | Yes |
| EQ | 100 | 50 | 22 wk | Low-Mod | None | Low | Moderate | Low | No |
| Tren | 500 | 500 | 22 wk | None | Very High | Low | Extreme | Low | No |
| Winny | 320 | 30 | 9 wk | None | None | High | Moderate | None | Yes |
| Anavar | 400 | 24 | 5 wk | None | None | Mild | Mild-Mod | Low | Yes |
| Mast | 96 | 33 | 12 wk | Anti-E | None | Low | Moderate | None | No |
| Primo | 88 | 50 | 6 wk | Minimal | Low | Low | Mild | Low | Yes |
| Adrol | 320 | 45 | 8 wk | None* | None* | Severe | Severe | Extreme | Yes |
| Dbol | 210 | 60 | 6 wk | High | Low | High | Mod-Sev | High | No |
* Anadrol: no aromatization, but estrogenic/gynecomastia effects are reported through an unclear mechanism. Ratings and detection windows are approximate and depend on dose, chronicity, method sensitivity, matrix, and individual pharmacokinetics.
Part IV: Forensic Detection Science
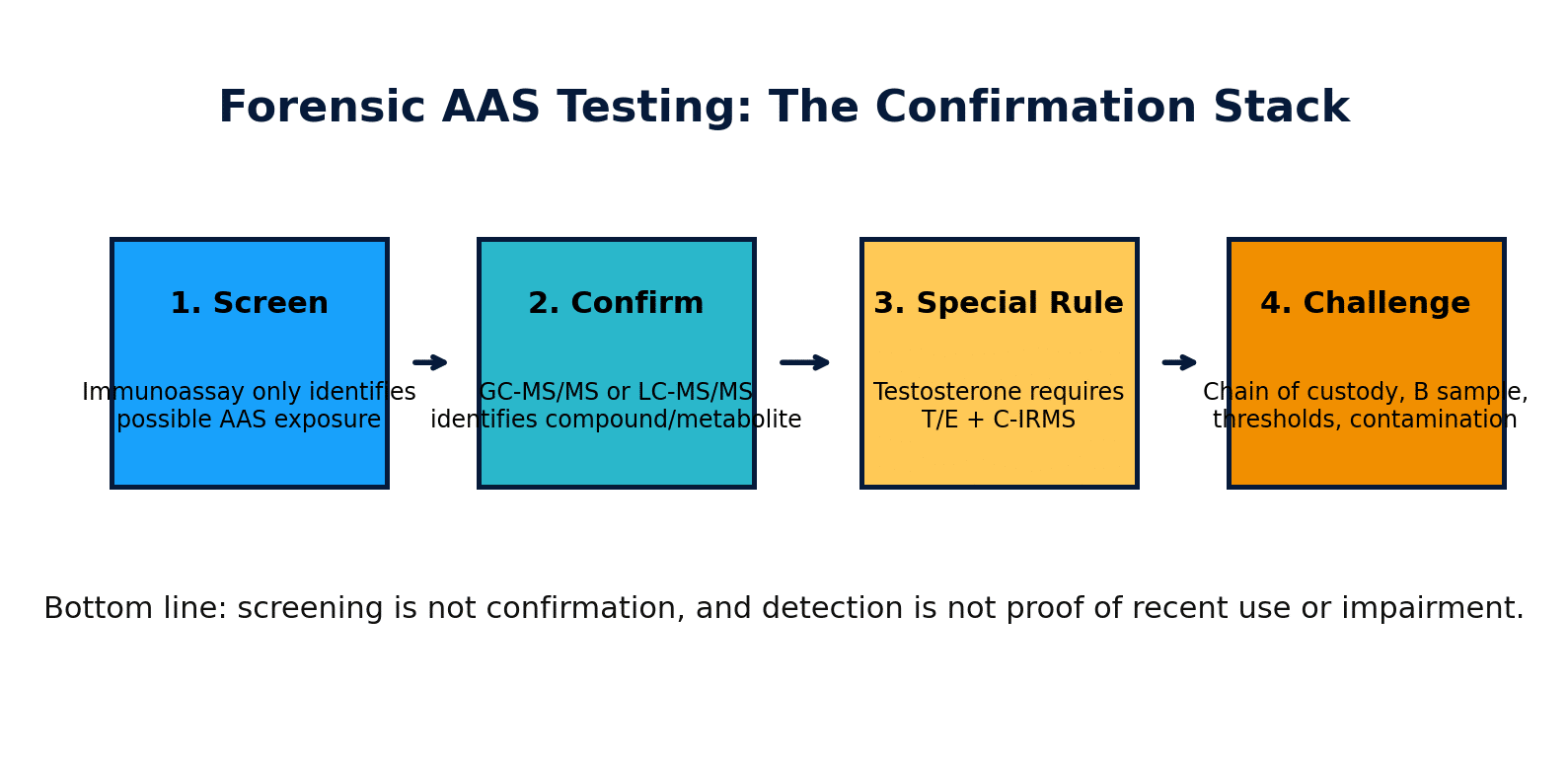
The Testing Stack
- Immunoassay screening: Fast and inexpensive, but prone to cross-reactivity. It is a screen only.
- GC-MS/MS: Core confirmation method for many AAS and metabolites; provides structural fragmentation data.
- LC-MS/MS: Preferred for polar, thermolabile, and some high-molecular-weight metabolites; important in modern anti-doping protocols.
- C-IRMS: Required when the question is whether testosterone or related endogenous steroids are synthetic/exogenous.
| The admissibility problem: A laboratory summary that says “positive” without showing screening method, confirmatory method, metabolite identity, threshold, uncertainty, and chain of custody is not a scientifically complete forensic report. |
Chain of Custody and Collection Questions
- Was the collection observed, and was specimen substitution reasonably excluded?
- Was temperature measured immediately at collection, and was it within physiological range?
- Were creatinine and specific gravity consistent with an authentic, non-dilute specimen?
- Was a split sample preserved, and can a B sample be tested?
- Was the laboratory properly accredited for the purpose asserted?
- Was the reported metabolite specific to the compound, or merely a class-level inference?
Common Defense Challenges in AAS Cases
| Issue | Why It Matters | Attorney/Expert Move |
| Supplement contamination | Some AAS positives can arise from contaminated over-the-counter products or precursors. | Demand quantitative levels, supplement history, lot testing, and literature-consistent contamination analysis. |
| Endogenous steroids | Testosterone and trace nandrolone issues can be endogenous or confounded. | Require IRMS or compound-specific metabolite confirmation before accepting exogenous-use opinions. |
| Detection window overreach | A positive result may reflect past exposure outside the relevant event window. | Compare the alleged timeline to ester, route, chronicity, dose, metabolite, and matrix. |
| Screening-only evidence | Immunoassay screens are not legally or scientifically equivalent to confirmation. | Demand chromatograms, method validation, uncertainty, calibration, and chain-of-custody documents. |
| Clinical leapfrogging | Presence is not impairment, aggression, intent, or causation. | Force the expert to identify human evidence connecting the compound, dose, timing, and behavior at issue. |
Conclusion
The forensic toxicology of anabolic-androgenic steroids is not a monolith. These ten compounds differ materially in structure, ester release, metabolite profile, detection window, hormonal activity, adverse-effect profile, and legal significance.
The central courtroom principles are consistent: screening is not confirmation; detection is not recent use; potency ratings are not impairment proof; testosterone requires isotope-ratio work; and long detection windows can be as exculpatory as they are incriminating when the alleged timeline does not fit the pharmacokinetics.
Attorney Checklist
- Obtain the full analytical packet, not only the summary result.
- Demand chain-of-custody documents from collection through analysis.
- Identify the exact compound and metabolite used for confirmation.
- For testosterone, confirm C-IRMS was performed; do not accept T/E ratio alone.
- Compare the alleged timeline with the compound’s ester, route, chronicity, and detection window.
- Review supplement contamination, endogenous production, and matrix-specific limitations.
- Attack any opinion that equates anabolic/androgenic ratings with impairment, aggression, or legal causation.



